紹介患者さんの経過観察。
以下の記事が治療時の記録である。
侵襲性の外部吸収であった。
あれからどうなっただろうか?
今日はその予後を時系列で整理してみる。
初診時主訴(2022.3.25)
左下奥歯隙間が大きく物が詰まりやすい(数年間)。CTで神経の周りが溶け出していると言われた。少し痛みはあるが薬を飲むまでもない。
初診時歯内療法学的検査(2022.3.25)
#18 Cold++3/4, Perc.(-), Palp.(-), BT(-), Perio Probe(WNL), Mobility(WNL)
#19 Cold+4/3, Perc.(-), Palp.(-), BT(-), Perio Probe(WNL), Mobility(WNL)
#18には強い痛みがある。
初診時PA(2022.3.25)

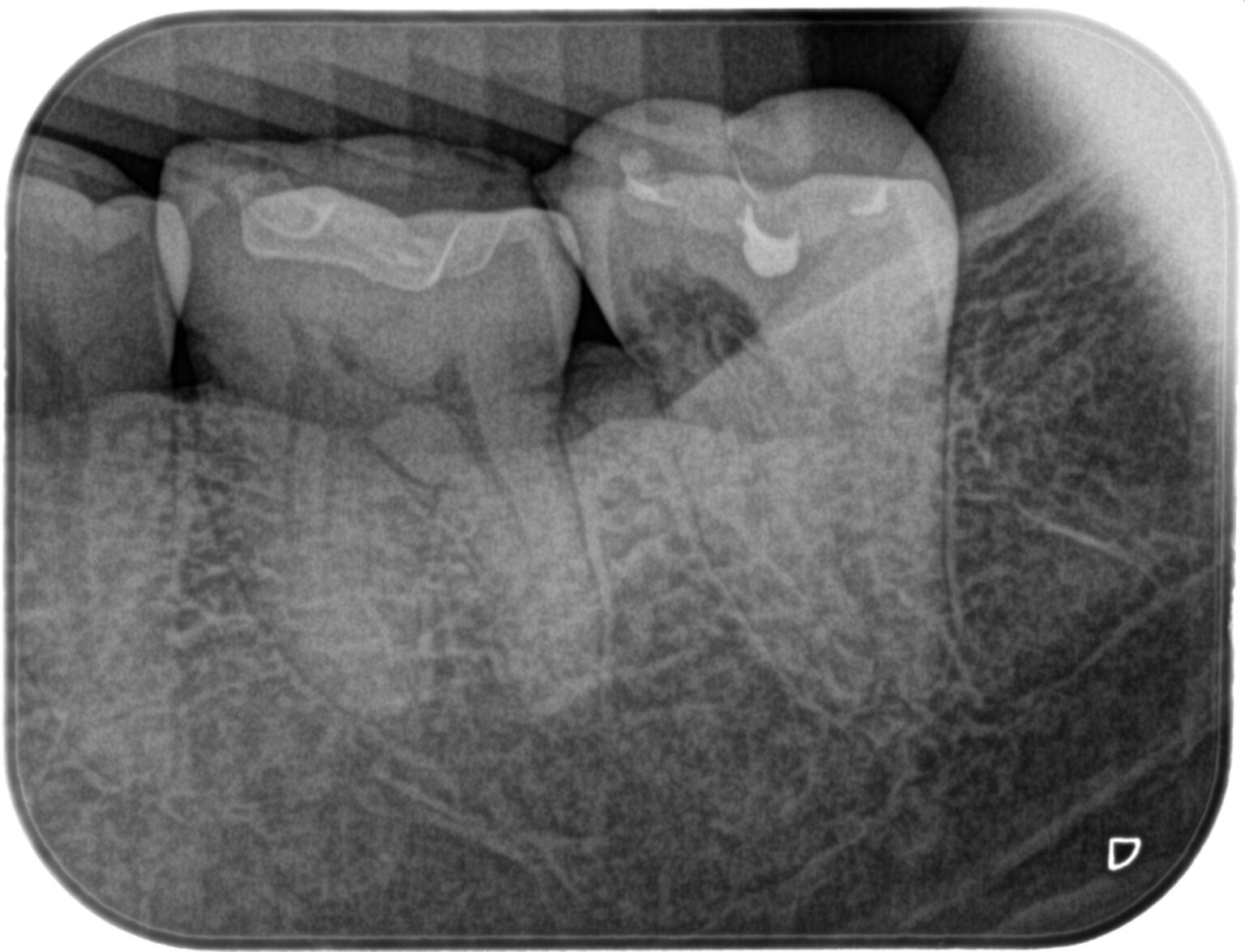
初診時CBCT(2022.3.25)

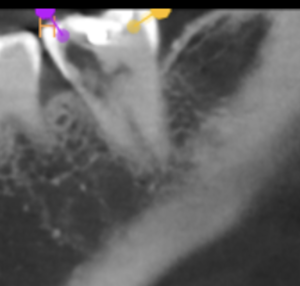

近心は既に外部吸収が進んでいるような絵の印象を与えている。
かつては、
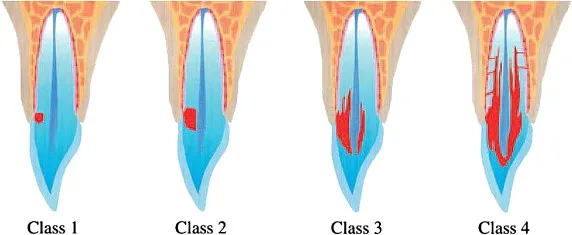
Heithersayの分類が多用されていた。
Success rate of ICRR
Heithersay 1999 Treatment of invasive cervical resorption: an analysis of results using topical application of trichloracetic acid, curettage, and restoration
それぞれの吸収における治療の成功率(3年予後)は以下である。
Class 1: 100%: Small, well-defined lesion localized to cervical area and involving dentin only.
Class 2: 100%: Slightly larger, well-defined lesion localized to cervical area but penetrating further into dentin close to the coronal pulp.
Class 3: 78%: Larger, less defined lesion extending into the coronal third of the root.
Class 4: 12.5%: Large lesion extending beyond the coronal third of the root.
次に彼が提唱する治療方法である。
Treatment of ICRR(Heithersay 1999c)
①Debridement of the resorptive defect(吸収部の機械的除去)
②Placement of glycerol on the gingival tissues, application of 90% trichloroacetic acid for 1 to 4 minutes(90% TCAの吸収部への塗布)
③Restoration with glass-ionomer cements(GICによる修復)
④To access the defect, a surgical flap is often necessary.(修復するには得手してFlap Opeが必要)
⑤Root canal therapy is indicated in class 2 and 3 defects because of inevitable pulpal involvement.(Class2,3ならば根管治療が必要)
⑥Trichloroacetic acid deactivates the resorptive tissue via coagulative necrosis.(TCAにより吸収組織を不活性化)
⑦Glass-ionomer cements are advised for restoration of resorptive defects because the ability of periodontal tissue to reattach to these materials.(GICで充填。歯周組織がくっつくので。)
⑧While generally an external approach is recommended for treatment an internal approach for repair can be undertaken for class 2 lesions and involves the use of intracoronal trichloroacetic acid or multiple applications of calcium hydroxide to assure clearance of resorptive soft tissue.(歯牙内部にTCAを塗布するか、水酸化カルシウムで貼薬するかする)
⑨Intentional replantation(意図的再植)
Heithersay (1999c) は、classes 1, 2, and 3の治療は推奨しているが、 Class 4 lesionsに関しては予後が悪いので保存をしないように推奨している。
吸収が広がるにつれて成功率が下がっている。
これは当たり前だ。
マネージメントができなかったからである。
そしてもう一つの重要なポイントが、この分類はCBCT出現以前のものであるという事実だ。
今は、以下のように変わっている。
Patel 2018 External cervical resorption/ a three-dimensional classification
Patel 2018 European Society of Endodontology position statement: External Cervical Resorption
Patel 2018 External cervical resorption-part 1: histopathology, distribution and presentation
Patel 2018 External cervical resorption: part 2 – management
これによれば以下のように分類されている。
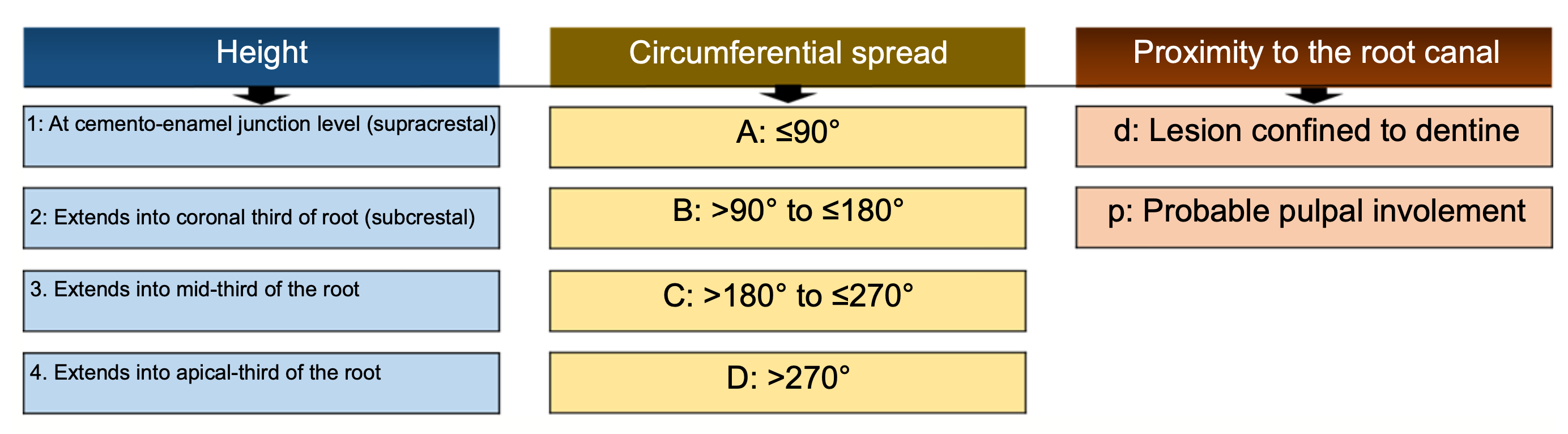
この分類によれば、
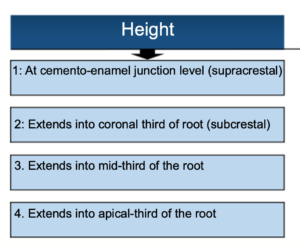
吸収の高さ(進行度具合)に関しては、2である。
次にどれくらい広がっているか?に関しては、
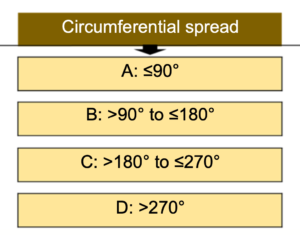
Cであると言える。
次に、吸収部分と歯髄の関係であるが、
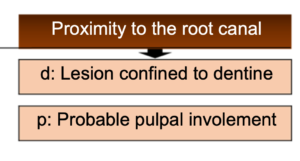
これは歯髄を含んでいると言って差し支えがないだろう。
以上を整理するとこの症例は、
2Bp(または3Bp)と言えるだろう。
さて、どのような治療を行うか?だが、
• External repair of the resorptive defect of endodontic treatment
Excavation of the resorptive defect and restoration of the defect with a direct restoration, for example Patel class 1Ad, 2Ad, 2Bd. Root canal treatment may be indicated if there is (probable) pulp involvement, for example Patel class 1Ap, 2Ap, 2Bp.
2Bpであれば根管治療+外部からの吸収のリペアが必要だという。
が、今日のケースで外部からFlapを開けて、直接法で吸収が取り切れるだろうか?
私には甚だ疑問である。
• Internal repair and root canal treatment
Root canal treatment, excavation and restoration of the resorptive defect with a direct plastic restoration, for example Patel class 2Cp, 2Dp, 3Cp, 3Dp.
内部からはこの症例に関してはリペアは不可能である。
• Intentional replantation
Extraction of an endodontically treated tooth to allow restoration and/or recontouring of an otherwise inaccessible ECR defect, followed by reinsertion.
Flapを開けてもアクセスができない位置に吸収がある場合、Intentional Replantationが提唱されている。今回はこれであろう。
• Periodic review
Untreatable teeth may be reviewed on a periodic basis, for example Patel class 2-4Dd, 2-4Dp.
吸収が歯をぐるっと回ってしまっていると保存ができない。経過を見るしかなさそうだ。
• Extraction
Indicated when ECR is inaccessible for treatment, or when the lesion is so extensive that the tooth may not be restored to satisfactory function or aesthetics.
吸収がひどく進行すると抜歯しかなくなる。
ということで、Intentional Replantationを行うことになるが、それを行うには、抜髄が必要である。
まず、根管治療を行い、築造後にIntentional Replantationを行うことになった。
#18 RCT+Core build up+Intentional Replantation(2022.6.14)
根尖病変がない歯なので、脱臼しないと抜歯ができない。
“脱臼”が最大のポイントだ。
樋状根でも…ここまで手をこまねいているのがわかる。
そして結局、#19の遠心を梃子にしないと抜歯は不可能だろう。
上記動画でそれがわかるだろうか?最後はダイヤモンド鉗子で抜歯した。
まさに…
パワープレイ
だ。
抜歯窩に落とし物がないことを確認し、歯牙を口腔外で観察した。
まずは、吸収部位の除去だ。
スプーンエキスカや手用器具では進まないので、途中でタービンに変えている。
この時に超音波スケーラーがあればもっと違ったと思われる。
が、2022.6.14の時点では市場にあの超音波は出回っていなかった。
今ならもっとやり方を変えただろう。
ということで、窩洞にこの時はBiodentineで埋めた。
グラスアイオノマー系のMTAであるということがその材料を選択したポイントだ。
もちろん、違う意見もあるだろう。

この後、Apicoectomyを行った。
Intentional Replantationの治癒をX線的に確認するためである。
逆根管形成を行った。
窩洞を乾燥し、逆根管充填した。またその後、吸収部位を埋めていたBiodentineに不安を覚えたため、BC puttyで追加で充填している。
12分で硬化するんじゃないのか?
メーカーの戯言?に我々はいつまで付き合わされるのだろうか?
この後、PAを撮影した。

コアの直下はBiodentineで、再表層がBC puttyだ。
特別それに(その構造に)問題はないと思われる。
抜歯窩を生食で洗浄し、再植した。
最後にPAを撮影した。
問題はないと思われる。
この後、経過を見せてもらうことになった。
#18 Intentional Replantation 2M recall(2022.8.30)


動揺はなく安定している。
プロビジョナルレストレーションを装着しても良さそうだ。
再植してから半年が経過した。
#18 Intentional Replantation 6M recall(2022.12.12)


最終補綴も問題なさそうだ。
ここからさらに時間が経過する。
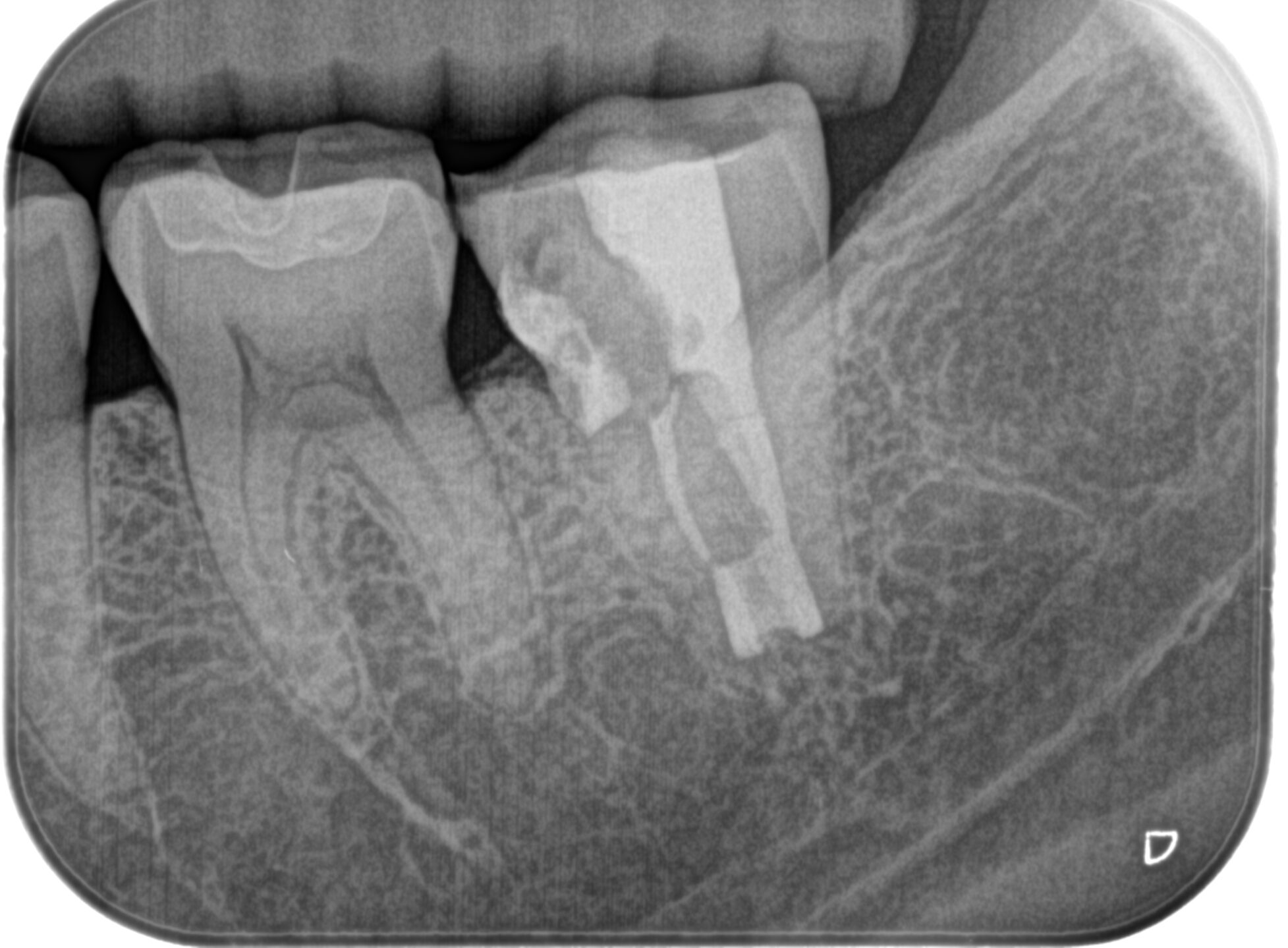
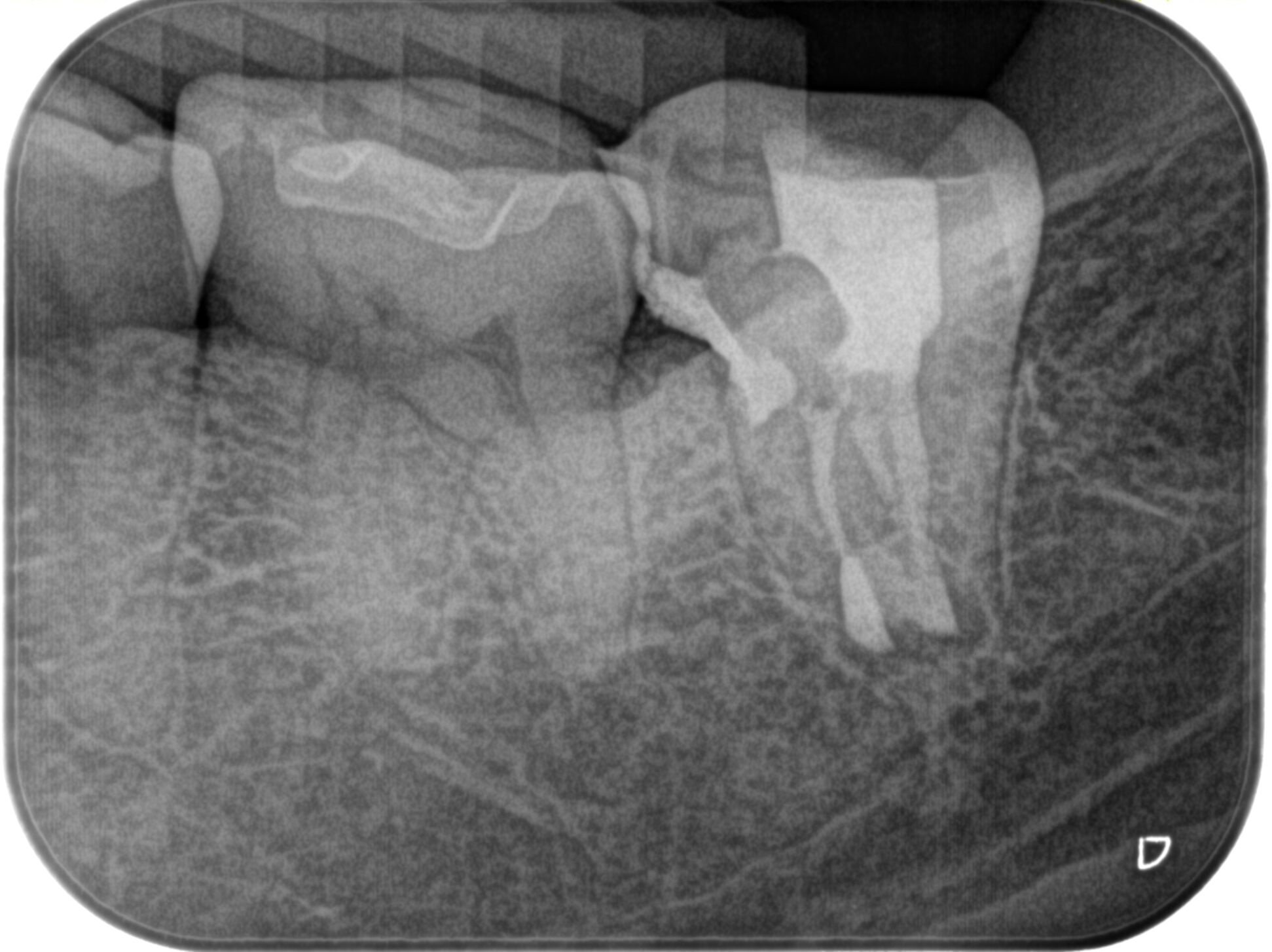
#18 Intentional Replantation 1.6yr recall(2023.12.20)
臨床症状は全くないという。
最終補綴も装着されていた。
PA, CBCTも撮影した。


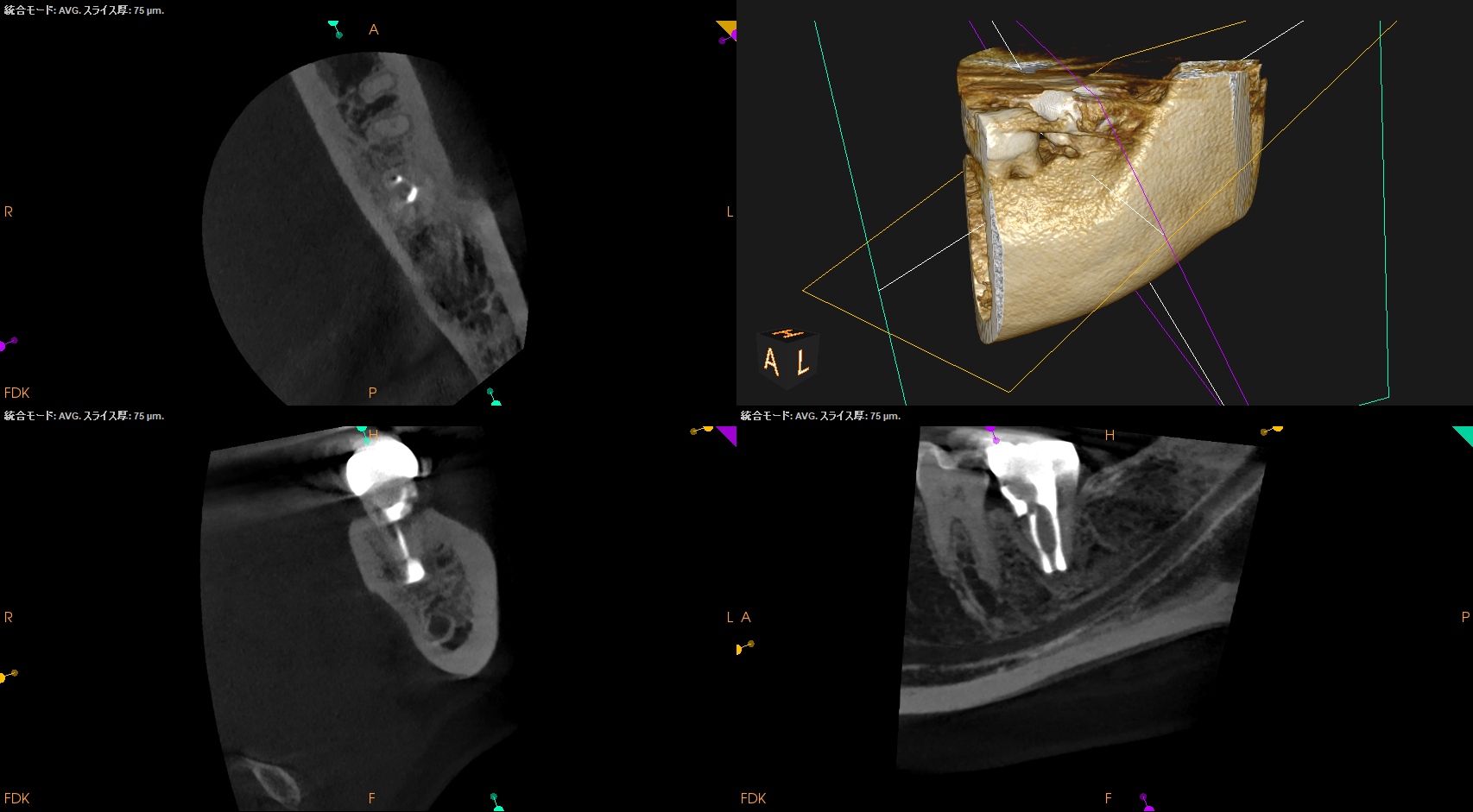
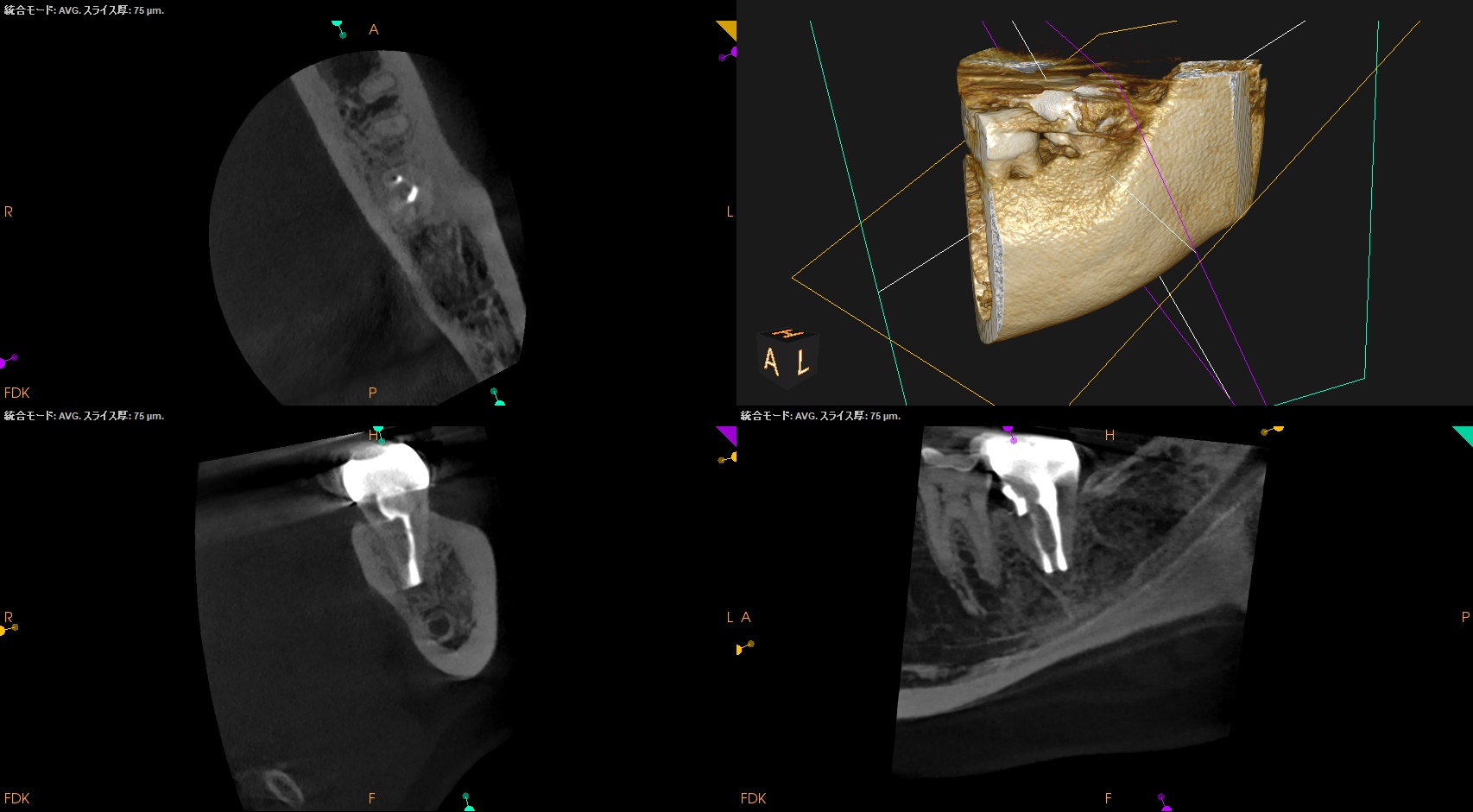
というところで今のところ問題ないと思われる。
次回は、1年後である。
また経過をご報告したい。