バイト先での治療。
患者さんは40代女性。
前歯に根尖病変があり、根管が石灰化しているという頭が痛い症例だ。
歯内療法学的診断は以下になる。
#6 Cold N/A, Perc.(-), Palp.(-), BT(-), Perio probe(WNL), Mobility(WNL)
#7 Cold NR/20, Perc.(+), Palp.(-), BT(+), Perio probe(WNL), Mobility(WNL)
#8 Cold N/A, Perc.(-), Palp.(-), BT(-), Perio probe(WNL), Mobility(WNL)
PAは以下になる。

歯内療法学的診断は以下になる。
#7
Pulp Dx: Pulp Necrosis, Periapical Dx: Symptomatic apical periodontitis
Recommended Tx: Apicoectomy(石灰化が高度に進んでいるため)
さてあなたはどの部位を治療するだろうか?
#8か?#7か?#7と#8か?
それはどのように決めるのか?と言えば、CBCTと臨床的な情報から総合的に考えて決定される。
近年の論文にその重要性を謳っていた?ものがある。
以下のような口腔内の状況である。
#6 Cold+(詳細なし), Perc.(-), Palp.(-), BT(-), Perio probe(WNL), Mobility(WNL)
#7 Cold+(詳細なし), Perc.(-), Palp.(-), BT(-), Perio probe(WNL), Mobility(WNL)
#8 Cold+(詳細なし), Perc.(-), Palp.(-), BT(-), Perio probe(WNL), Mobility(WNL)
PAと口腔内写真である。

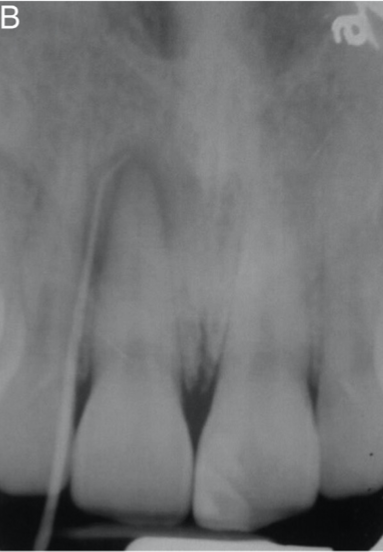
Sinus tractがあるのに、#8はCold(+)である。
???
なぜだろうか?
あなたの検査の方法が悪かったのだろうか?
それとも他に問題があるのだろうか?
こういう診断に整合性が得られないときは、CBCTを利用することを一般的に薦められている。
CBCTを撮影した。
CBCT imaging revealed a low-density area partially surrounded by a high-density (corticated) area, which appeared as a widening of the nasopalatine duct
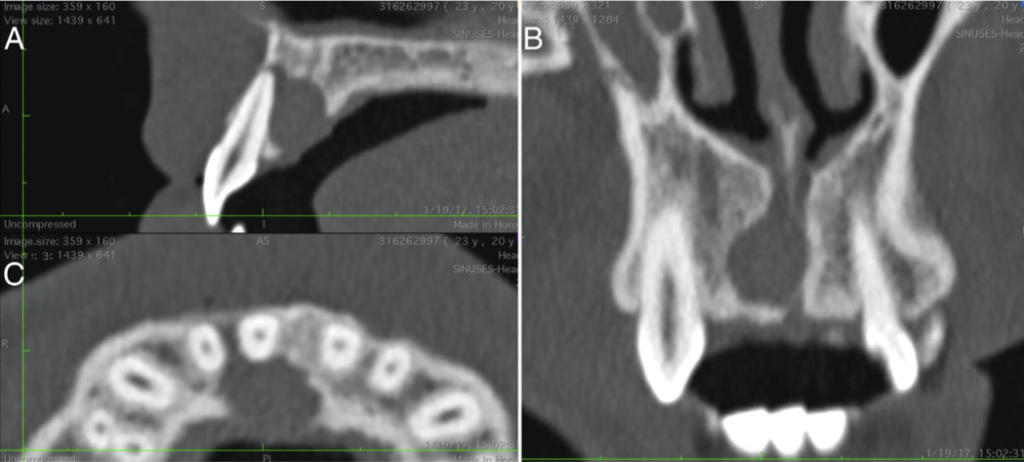
The lesion, which was somewhat asymmetrical and irregularly shaped, perforated the palatal and, to a much lesser extent, the buccal cortical bone plates of the alveolar process.
Nasopalatine cystを疑った著者は口蓋から外科治療を行い、嚢胞状物質を生検に出した。
すると以下のような結果が返ってきたのである。
The histopathologic findings were an inflamed cyst with an upper respiratory–type and stratified squamous epithelium with adjacent mucous glands. In addition, a large colony of Actinomyces spp. was found surrounded by an inflammatory infiltrate in a typical “sunray” appearance, which is consistent with an active Actinomycosis infection. These findings are consistent with the diagnosis of an infected Nasopalatine Duct Cyst.
つまり、Apicoectomyをせずに鼻口蓋管嚢胞と疑って口蓋からフラップを開けたために余計な治療を行わなくて済んだのである。
つまり、著者はCBCTのお陰であると結論づけている。
しかし私から言わせれば、#8はCold(+)になった時点で根管治療の対象にはならないだろう。
もしこれを非外科的にことを薦めていくのであれば…
生検以外にそれを調査する方法はない。
したがってかなり賭けの要素も強い処置になったと言えるだろう。
でもCBCTがあれば鼻口蓋管嚢胞と疑うことができる。
それが大事なのである。
ということで診断にはCBCTは欠かせないものであるということは論を待たない。
その他の臨床情報としては、
NPDC is the most common nonodontogenic cyst in the maxilla and therefore should always be suspected in cases of radiolucency in the maxillary incisor area.
The pulp of adjacent teeth will usually stay vital even in large NPDCs.
この辺りが決定打になるのだろう。
ということで、CBCTは臨床上有効である。
で、この症例であるがいかがだろうか?
#8の右に存在するのは曩胞か?それとも鼻口蓋管か?
と言えば、CBCTが役に立つのでその情報を見てみよう。
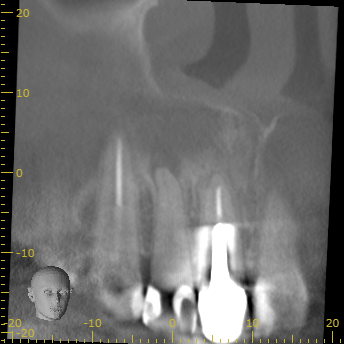
ということで、#8の右に存在するのは鼻口蓋管と考えられる。
#7は石灰化が高度に進んでいるために外科治療(Apicoectomy)となった。

ということで外科治療は30分以内で終了した。
次回は半年後に経過観察である。
治療にはそれを役立ててくれるアイテムがあるのできちんと使いこなしていこう。
道具に使われるのではなく、道具を使いこなすのだ。
