
7歳の女児。
セミナーに出ている先生からの紹介で県外から来院された。
主訴は前歯部の主張と失活にともなう根の未閉鎖(紹介された歯科医師の主訴かもしれない。)
歯内療法学的検査をおこなった。
#8 Cold+1/3, Perc.(-), Palp.(-), BT(-), Perio Probe(WNL), Mobility(WNL)
#9 Cold N/A, Perc.(-), Palp.(+), BT(-), Perio Probe(WNL), Mobility(WNL), Sinus tract(+)
#10 Cold+2/2, Perc.(-), Palp.(-), BT(-), Perio Probe(WNL), Mobility(WNL)
PAは以下になる。


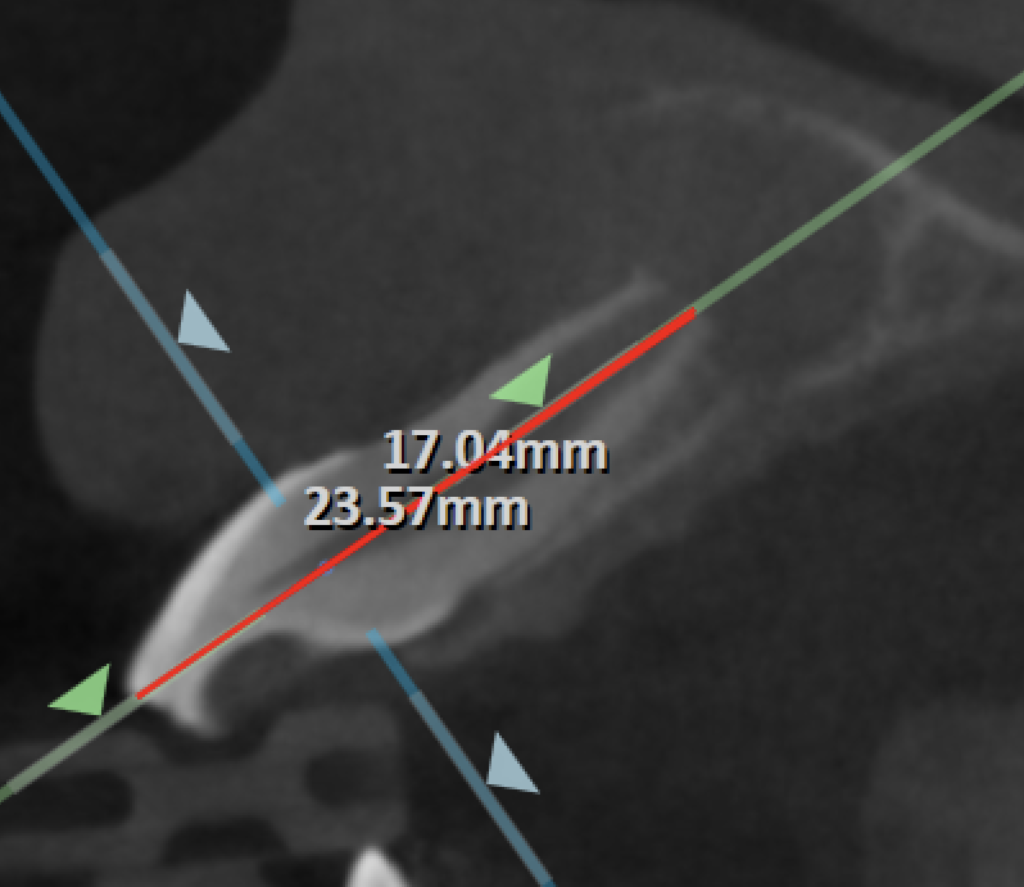
歯根の長さは左右対称であることから、歯根が太くなる前に歯髄が失活してしまったのだろうということが予想できる。
また、CBCTも撮影した。
以上から歯内療法学的病名は以下になる。
Pulp Dx: Pulp Necrosis
Periapical Dx: Chronic apical abscess
Recommended Tx: Regenerative Endodontics
Regenerative Endodonticsについてご両親に説明した。
AAEの治療に関するInformed Consent を参考にしている。
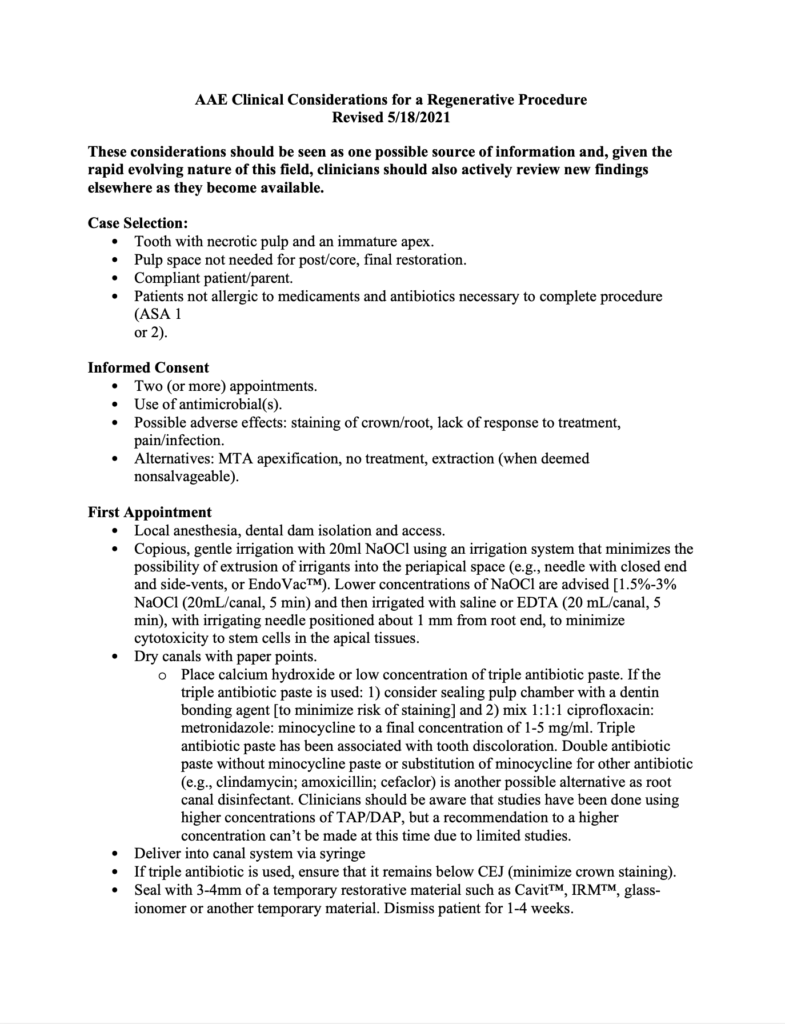
AAE Clinical Considerations for a Regenerative Procedure Revised
2021.5.18に改訂されている。
改訂は定期的にされているが、ほとんど変更はない。
そして各種エビデンスが低すぎる。
主な要点は以下になる。
These considerations should be seen as one possible source of information and, given the rapid evolving nature of this field, clinicians should also actively review new findings elsewhere as they become available.
序文に記されている言葉はこのガイドを参考に治療しなさいと書いてあるが、新しい発見が出てくればそれは何でもreviewしなければならないと書いてある。
いつまでも過去の遺物に拘る日本とアメリカの歯科医療の大きな違いが、ここである。
さらに読み進めていく。
Case Selection:
• Tooth with necrotic pulp and an immature apex.(歯髄壊死した根未完成歯)
• Pulp space not needed for post/core, final restoration.(ポストやコアや最終補綴が不要な症例)
• Compliant patient/parent.(協力性がある患者さん)
• Patients not allergic to medicaments and antibiotics necessary to complete procedure, ASA 1 or 2.(ASA1か2の健康な患者さん)
Informed Consent
• Two (or more) appointments.(2回以上のアポイントが必要な可能性)
• Use of antimicrobial(s).(抗生物質を使用することがある。3Mixのことである。)
• Possible adverse effects: staining of crown/root, lack of response to treatment, pain/infection.(歯牙の変色、治療、痛み・感染に対して反応しない可能性)
• Alternatives: MTA apexification, no treatment, extraction (when deemed non salvageable).(代替治療:MTAアペキシフィケーション, 治療しない, 抜歯)
First Appointment
• Local anesthesia, dental dam isolation and access.(麻酔、ラバーダム、アクセスプレパレーション必要)
• Copious, gentle irrigation with 20ml NaOCl using an irrigation system that minimizes the possibility of extrusion of irrigants into the periapical space (e.g., needle with closed end and side-vents, or EndoVac). Lower concentrations of NaOCl are advised [1.5%-3% NaOCl (20mL/canal, 5 min) and then irrigated with saline or EDTA (20 mL/canal, 5 min), with irrigating needle positioned about 1 mm from root end, to minimize cytotoxicity to stem cells in the apical tissues.(20mlの1.5~3%のヒポクロで洗浄。Closedのニードルが望ましい。またはEndoVac使用。その後、20mlのEDTAで根管を洗浄する)
• Dry canals with paper points.(ペーパーポイントで根管を乾燥)
• Place calcium hydroxide or low concentration of triple antibiotic paste. (水酸化カルシウムか3Mixを根管に貼薬)
• Seal with 3-4mm of a temporary restorative material such as CavitTM, IRMTM, glass-ionomer or another temporary material. Dismiss patient for 1-4 weeks.(Caviton等で仮封し、1~4週間後に経過観察する)
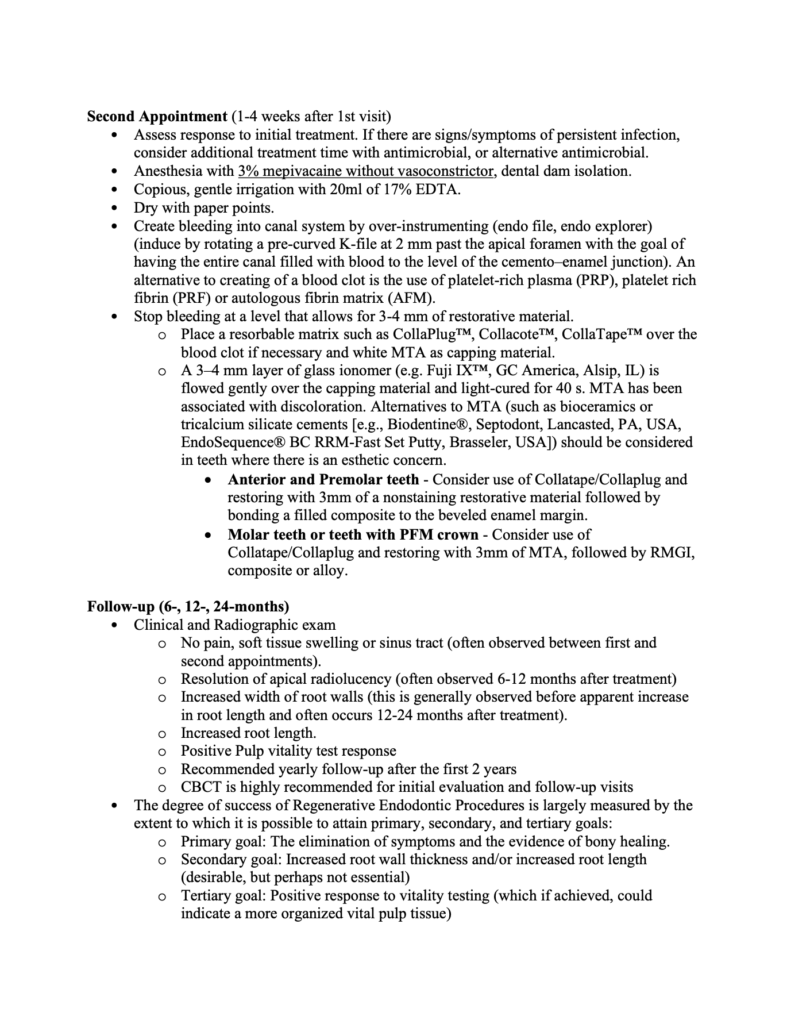
Second Appointment (1-4 weeks after 1st visit)
• Assess response to initial treatment. If there are signs/symptoms of persistent infection, consider additional treatment time with antimicrobial, or alternative antimicrobial.(1回目の治療の評価をする。もし問題があれば再度洗浄を行うかこの治療自体を止めるかどちらか。)
• Anesthesia with 3% mepivacaine without vasoconstrictor, dental dam isolation.(3%メピバカイン=3%スキャンドネストを使用)
• Copious, gentle irrigation with 20ml of 17% EDTA.(20mlのEDTAで洗浄)
• Dry with paper points.(ペーパーポイントで根管乾燥)
• Create bleeding into canal system by over-instrumenting (endo file, endo explorer) (induce by rotating a pre-curved K-file at 2 mm past the apical foramen with the goal of having the entire canal filled with blood to the level of the cemento–enamel junction). An alternative to creating of a blood clot is the use of platelet-rich plasma (PRP), platelet rich fibrin (PRF) or autologous fibrin matrix (AFM).(オーバー形成して根管内に血液を送る)
• Stop bleeding at a level that allows for 3-4 mm of restorative material.(修復部位の3~4mm直下で止血させる)
• Place a resorbable matrix such as CollaPlug, Collacote, CollaTape over the blood clot if necessary and white MTA as capping material.(コラプラグ、コラテープ、コラコートなどの材料を出血の上に置く)
• A 3–4 mm layer of glass ionomer (e.g. Fuji IXTM, GC America, Alsip, IL) is flowed gently over the capping material and light-cured for 40 s. MTA has been associated with discoloration. Alternatives to MTA (such as bioceramics or tricalcium silicate cements [e.g., Biodentine®, Septodont, Lancasted, PA, USA, EndoSequence® BC RRM-Fast Set Putty, Brasseler, USA]) should be considered in teeth where there is an esthetic concern.(MTAの上に修復材料を置く。変色が気になれば、BiodentineやBC puttyを用いる。)
• Anterior and Premolar teeth – Consider use of Collatape/Collaplug and restoring with 3mm of a nonstaining restorative material followed by bonding a filled composite to the beveled enamel margin.(前歯→最終的にはCRで充填)
• Molar teeth or teeth with PFM crown – Consider use of Collatape/Collaplug and restoring with 3mm of MTA, followed by RMGI, composite or alloy.(臼歯→CRか金属修復へ)
Follow-up (6-, 12-, 24-months)
• Clinical and Radiographic exam(臨床検査・レントゲン検査必要)
①No pain, soft tissue swelling or sinus tract (often observed between first and second appointments).(痛みや軟組織の腫脹がないあるいはSinus tractが消失。これはしばしば1回目と2回目の治療の間に起きることが多い)
②Resolution of apical radiolucency (often observed 6-12 months after treatment) (根尖病変の喪失。しばしば治療後6~12ヶ月で生じることが多い)
③Increased width of root walls (this is generally observed before apparent increase in root length and often occurs 12-24 months after treatment).
(根管長と根管壁の増大. 治療後12~24ヶ月で起きることが多い)
④Increased root length.(歯根の成長)
⑤Positive Pulp vitality test response(Cold test等に対する陽性反応)
⑥Recommended yearly follow-up after the first 2 years(術後2年の最低限の経過観察)
⑦CBCT is highly recommended for initial evaluation and follow-up visits(CBCTの撮影)
• The degree of success of Regenerative Endodontic Procedures is largely measured by the extent to which it is possible to attain primary, secondary, and tertiary goals:
①Primary goal: The elimination of symptoms and the evidence of bony healing.(第1のゴール:症状の喪失と根尖病変の治癒)
②Secondary goal: Increased root wall thickness and/or increased root length(desirable, but perhaps not essential)(第2のゴール:根管壁・歯根の成長。理想的だがマストではない)
③Tertiary goal: Positive response to vitality testing (which if achieved, could indicate a more organized vital pulp tissue)(第3のゴール:生活反応の獲得)
以上がAAEのRegenerationに対する指針である。
私が知る限り、
違和感があるのが青地で記した部分
である。
まず1.5~3%のヒポクロだが、化学者でもない我々がどうやってそれを得ろと言うのだろうか?
非常に難しいだろう。
今でもこの手の話になると、ヒポクロの瓶の後ろの記述を思い出す。


また、3%メピバカイン=3%スキャンドネストを使用
であるが、これは前歯には無理な話だ。
5~10分で効果が切れる麻酔を使用して上顎前歯のRegenerationを小児にマネージメントすることは事実上、無理といっていい。
しかもこのスキャンドネスト使用しなさい、と言う勧告はCase Reportである。
Petrino 2009 Challenges in Regenerative Endodontics: A Case Series
2回目の治療にキシロカインを使用したら、出血がなかったのでスキャンドネストを使用しました、と言う論文に重いエビデンスがあるだろうか?
私にはそうは思えない。
また、第3のゴールである”生活反応の獲得”だが私はこれは起きないと思っている。
あくまでも経験的だが…
ということで以上のような説明をし、親御さんが治療に同意されたので歯科治療が行われたが…
子供は号泣であった。。。
それはそうだ。
訳もわからず博多の歯科医院に連れて行かれて、
いきなり麻酔をされて(歯科治療などしたことがない)、
ゴムのシートを付けられて、
歯に穴を開けられて、
洗浄させられ、
水酸化カルシウムを貼薬されるのである。
私も水酸化カルシウムを久々に使用した。
この治療以外に使い所がないからだ。
1回目の治療が終わり、2回目は1ヶ月後に予約をとられた。
それがこの日(2021.12.28)であった。
EDTA 20mlで根管内を洗浄する。
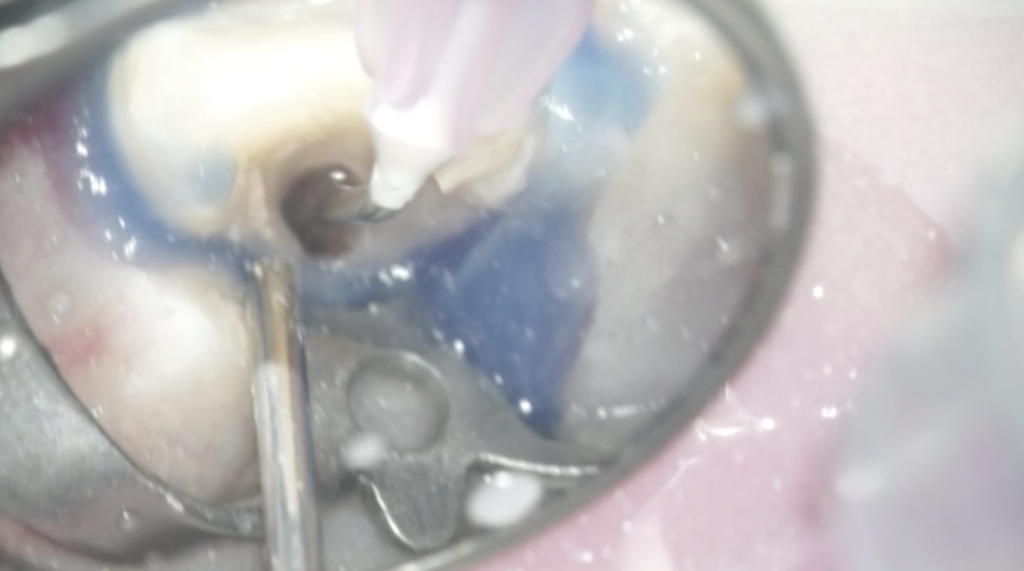
その意味は
EDTA promotes exposure of growth factors in dentin, differentiation of stem cells into
odontoblast like cells and adhesion of those cells to dentin.
EDTAは根管壁をエッチングしてStem cellを象牙芽細胞に分化させる
のである。
そして、根管内をペーパーポイントで乾燥し

ファイル(K#35,#30,#25)の先端をベンドして根管に挿入し、根尖へ突き出して出血を促した。

この治療のメイン・イベントになる部分である。
キシロカインを使用したが…出血はきちんと起こっている。
そして久々使用したColla-Plugを血餅の上に置いて、

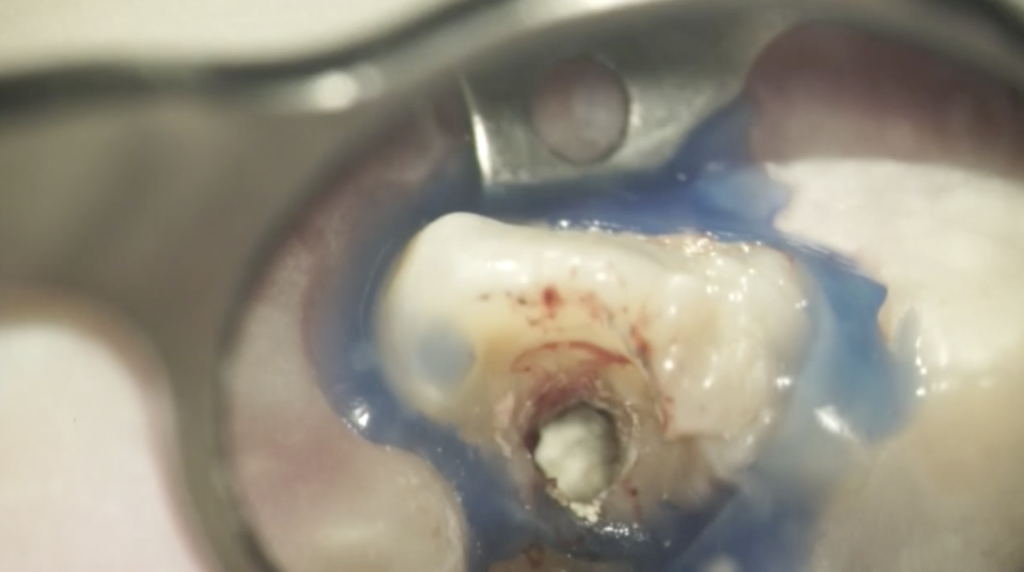
その上にBC Puttyを置いてCR充填して封鎖した。

治療後にデンタル撮影をおこなった。
以下になる。


次回は半年後に、歯内療法学的検査とPA撮影である。
そして1年後に、歯内療法学的検査、PA撮影、CBCTである。
さらに1年後に、歯内療法学的検査、PA撮影、CBCTである。
ということでこの日の治療が終了した。
経過観察では、上で既に記した
①Primary goal: The elimination of symptoms and the evidence of bony healing.(第1のゴール:症状の喪失と根尖病変の治癒)
②Secondary goal: Increased root wall thickness and/or increased root length(desirable, but perhaps not essential)(第2のゴール:根管壁・歯根の成長。理想的だがマストではない)
③Tertiary goal: Positive response to vitality testing (which if achieved, could indicate a more organized vital pulp tissue)(第3のゴール:生活反応の獲得)
などをcheckする。
長い戦い(と言っても30分もかかっていないが)は終了した。
このように、
私は(当歯科医院は)子供の治療も行っている。
USCの時の、PEDO Timeを思い出す。
毎週1回の生贄時間であった…
今回の子は治療は上手であったが、麻酔をするとか、途中で痛くなるとかそういうのがNGで途中、何回か号泣して治療の完了が危ういところだった。
しかしまあこれは、
1回目の治療はSinus tractがあったっことから麻酔が切れやすく治療途中に痛みが出やすいといえるが、
2回目はSinus tractは消失したため痛みは出にくいといえる。
ということで、今回もこの子はよく頑張った。
さて、皆さんは次回の経過観察をお待ちいただきたい。