紹介患者さんの治療。
主訴は、
子供がこけて、前歯を打って歯の神経が死んでしまっていると言われた…治療をお願いしたい
であった。
ちなみに患者さんは小学3年生の女児である。
うちの歯科医院は年に数人、子供が来る。
子供の治療は、勤務医時代とUSC時代に鍛えられた。
私は得意ではないとか得意だとかそうは言えないのが当時の状況であった。
あれから8年。
私は再び、子供と向き合うことになる。
歯内療法学的検査(2023.11.29)
#8 Cold+2/2, Perc.(-), Palp.(-), BT(-), Perio Probe(WNL), Mobility(WNL)
#9 Cold+1/3, Perc.(-), Palp.(-), BT(-), Perio Probe(WNL), Mobility(WNL)
#8も依頼された#9もCold Testに反応している。
そのことから、
神経を取る必要がないのではないか?という意見が出てくるだろう。
なぜこのような
不思議な現象?が起きるのだろうか?
それは後ほど説明しよう。
PA, CBCTも撮影した。
PA(2023.11.29)


PAでは正直、
???
である。
もはやPAはその存在意義をあまり感じさせないものになってしまっていると言っていいだろう。
ということで、CTも撮影した。
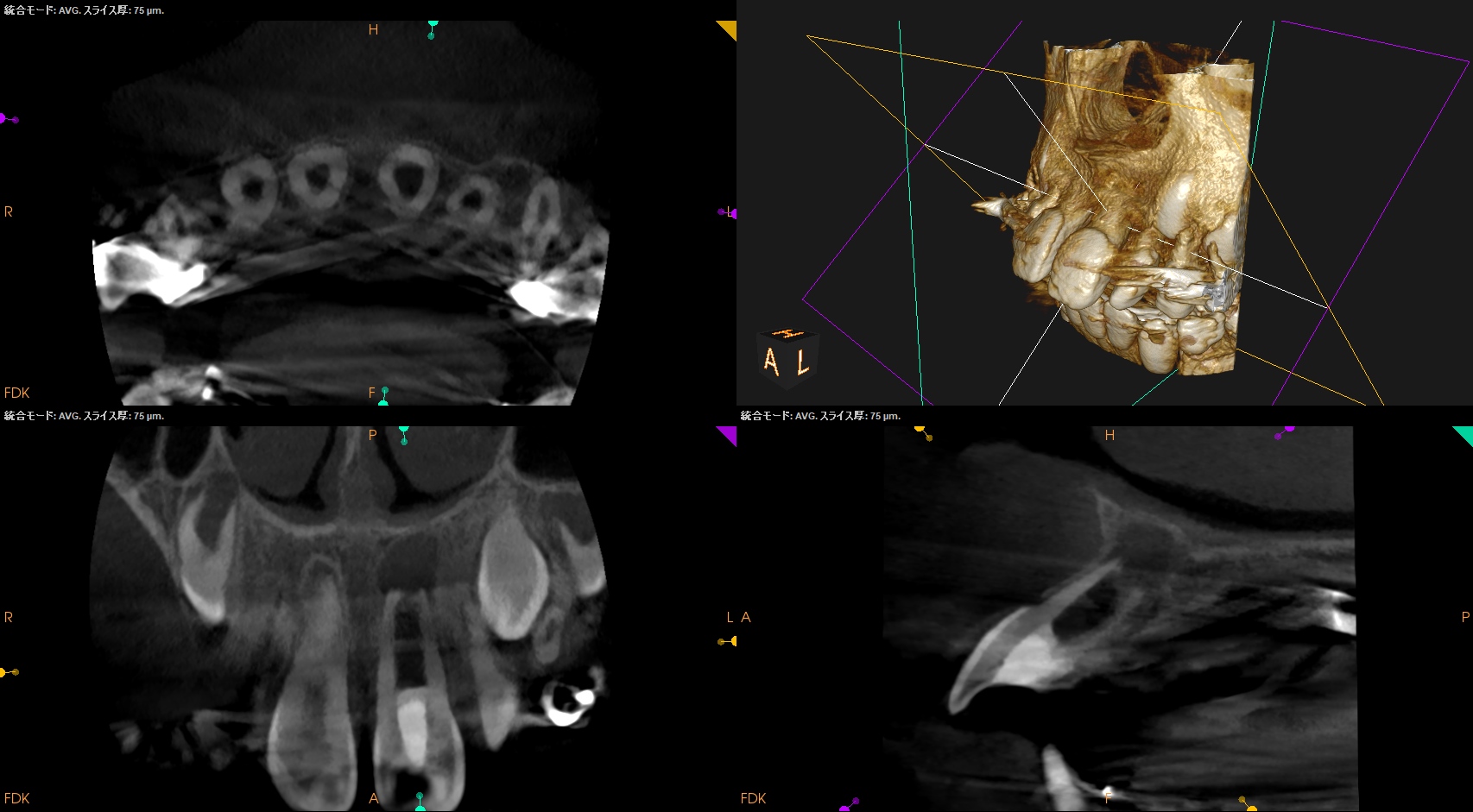
CBCT(2023.11.29)
#9
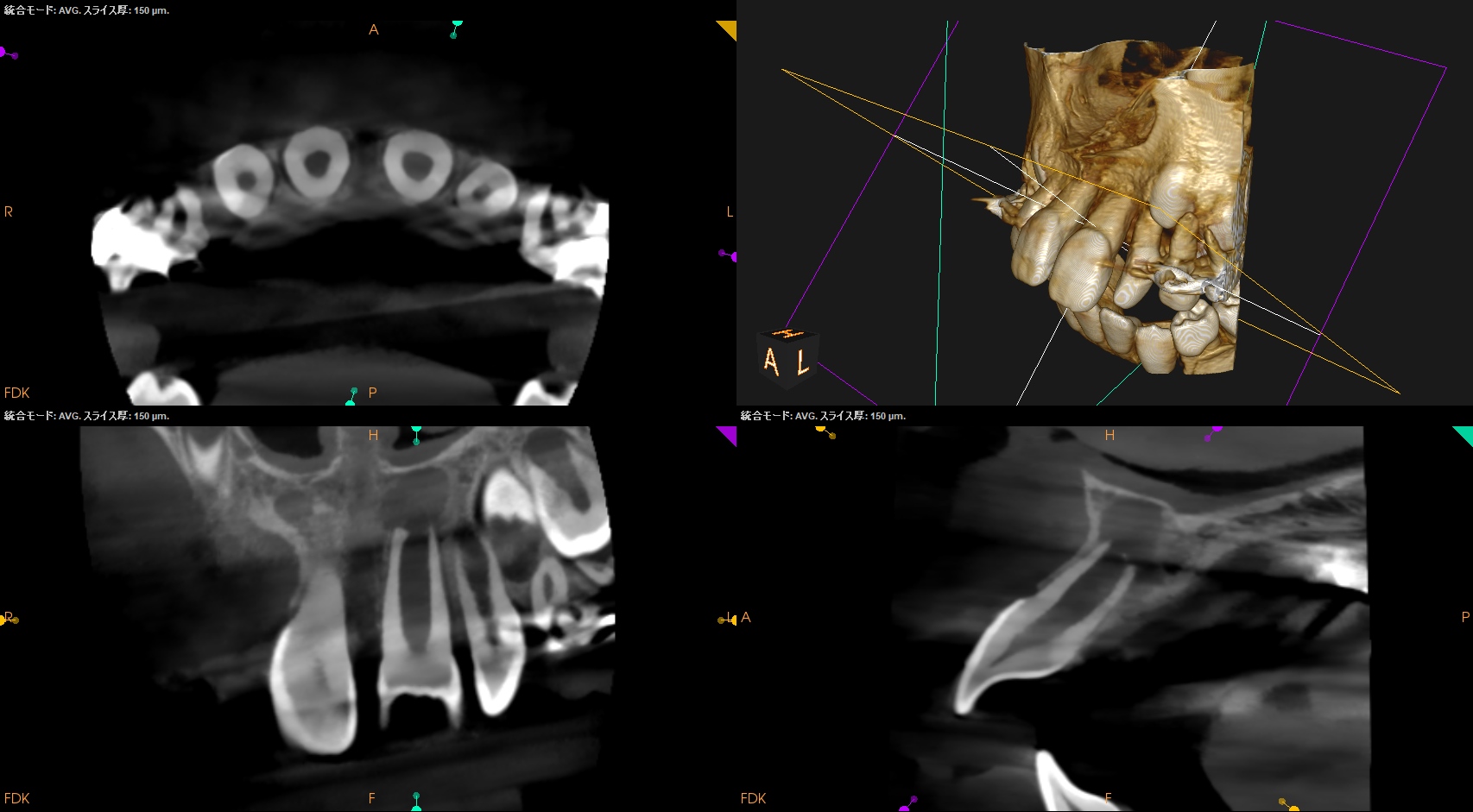
これだけ見ても???だろう。
この手の治療は必ず、
反対側同名歯
も見なければならない。
#8
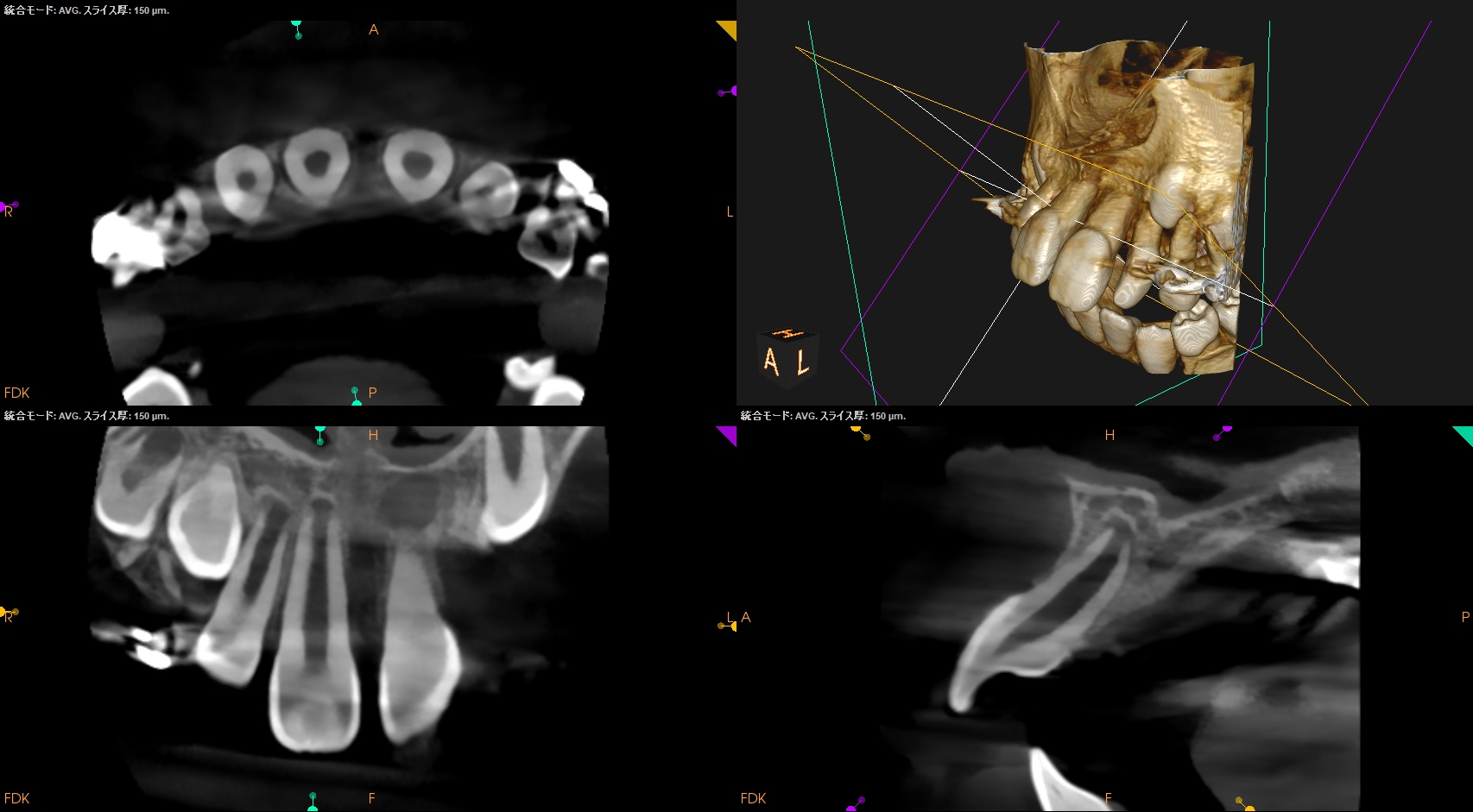
#8と#9を比べてみよう。

#9は自傷事故で歯髄が壊死した可能性が高い。
#8と比べるとその違いがわかるだろう。
ではなぜ、#9はCold testに反応するのだろうか?
といえばそれは、2つ原因がある。
1つは、
学術的にはA∂繊維(冷たいものを冷たいですよ、と脳に伝える神経繊維)が髄角付近に残存しているから
と考えられている。
Coldを中枢神経に伝える主たる神経繊維であるA∂繊維は髄角付近にある。それは壊死しても消えていない。
ということは…Cold testに反応するのだ。
この話は、まさにBasicで知らないといけないが、実際はAdvanced的な内容である。
大学の基礎系の授業で習う内容は実は全てAdvanced的な内容であるという事実。
歯科医療は簡単なようで難しい?のか??
さてもう一つの理由はといえば、
患者(小学生)の冷たい刺激に対する過度な反応
である。
何でも手が上がるというやつだ。
AAEも“そこまで”想定していないことは容易だ。
しかし、臨床的にそれがどちらであれ治療はしなければならないことは間違い無いだろう。
歯内療法学的診断(2023.11.29)
Pulp Dx: Pulp Necrosis
Periapical Dx: Symptomatic apical periodontitis
Recommended Tx: Regeneration
ということで、推奨される治療は再生(的)療法だ。
歯髄の再生はないが、再生に近い形でゴールを迎えるというこの治療は過去(私の大学院生時代)熱い?治療であったが、最近では落ち着いてきただろう。
現状、アメリカ歯内療法学会(AAE)のこの手の治療のゴールは以下にある通りだ。
AAE Clinical Considerations for a Regenerative Procedure Revised 5/18/2021
The degree of success of Regenerative Endodontic Procedures is largely measured by the extent to which it is possible to attain primary, secondary, and tertiary goals:
▶︎ Primary goal: The elimination of symptoms and the evidence of bony healing.
▶︎ Secondary goal: Increased root wall thickness and/or increased root length(desirable, but perhaps not essential)
▶︎ Tertiary goal: Positive response to vitality testing (which if achieved, could indicate a more organized vital pulp tissue)
3つ目のゴールである、
Cold testに反応することであるが、こんなことは決して起きないだろう。
あるとすれば、恐怖から手が上がるくらいだろう。
頼むよ、AAE…
これも前述した内容の通りだ。
さて。
近年は、再生(的)療法も1回法が提唱されている。
以下である。
<Regeneration 1回法>
カンピーナス州立大学(他の州立大学よりも潤沢な予算が配分されており、贅沢な設備と教授陣が特徴である。このため入学希望者は多く、ブラジルで最も入学困難な大学といわれている)の が、以下の術式で1回法と2回法のRegenerationを行なっている。
2回法
1回目
局所麻酔 (特に指定なし)
ラバーダム防湿
アクセスキャビティ
作業長決定
20ml 1.5-3% ヒポクロ /5分(サイドベントもしくはEndo Vac推奨)
20ml 生食もしくはEDTA /5分
ペーパーポイント乾燥
根管内貼薬 (水酸化カルシウム製剤 もしくは シプロフロキサシン、メトロニダゾール、ミノサイクリンの3剤=3Mix 混和)
Cavit、IRM、GICなどで仮封
2回目
局所麻酔 (10万倍希釈エピネフリン含有2%キシロカイン)
ラバーダム防湿
アクセスキャビティ
作業長決定
10ml 生食
3ml 17% EDTA
5ml 生食
ペーパーポイント乾燥
足場としての血餅
コラーゲン繊維
歯頚部バリア (水酸化カルシウム製剤、2%クロルヘキシジンジェル、酸化亜鉛を混和)
Coltosol (根管口部仮封)
コンポジットレジン 充填(アクセスキャビティ)
驚くことに、2回目もキシロカインで麻酔している。
その心は、
スキャンドネストであれば麻酔がすぐ切れるから
だ。
私は事実上、スキャンドネストでRegenerationを行うのは不可能であると考える。
それをするくらいなら、1回法で終わった方がマシだともいえなくない。
ちなみに
AAEの推奨するRegenerationの術式(2021.5.18が最新版)
は2回法で以下だ。
1回目
局所麻酔 (特に指定なし)
ラバーダム防湿
アクセスキャビティ
作業長決定
20ml 1.5-3% ヒポクロ /5分(サイドベントもしくはEndo Vac推奨)
20ml 生食もしくはEDTA /5分
ペーパーポイント乾燥
根管内貼薬 (水酸化カルシウム製剤 もしくは シプロフロキサシン、メトロニダゾール、ミノサイクリンの3剤混和)
Cavit、IRM、GICなどで仮封
2回目
局所麻酔 (3%スキャンドネスト)
ラバーダム防湿
アクセスキャビティ
20ml 17% EDTA
ペーパーポイント乾燥
オーバーインスツルメンテーションで出血させて血餅を作る
CollaPlug、Collacote、CollaTapeなどの吸収性物質を静置
必要であればMTAセメントを留置(MTAの代わりに、BC puttyやBiodentineを使用しても問題ない)
3~4mmの深さをGICなどで封鎖
あなたはなぜ、2回目がスキャンドネストかご存知だろうか?
実は、非常にしょうもない理由である。
エビデンス的にはCase Reportレベルの内容だ。
これでそれを使わせるのか?的な内容で閉口してしまう。
が、この文献ではキシロカインを使用していた。
これは仕方がないだろう。
IEJでははっきりとは言わないまでも、
スキャンドネストでRegenerationを行うことの難易度の高さ(麻酔が効かないという面の欠点)を取り上げていた。
もはや、この治療はキシロカインで行うものだという認識が私にはある。
その際の注意点は、治療をさっさと進めていくということである。
たらたら治療していては止血作用が出て、はいまた来てください!になりかねないからだ。
ということでこの研究の結果は以下だ。
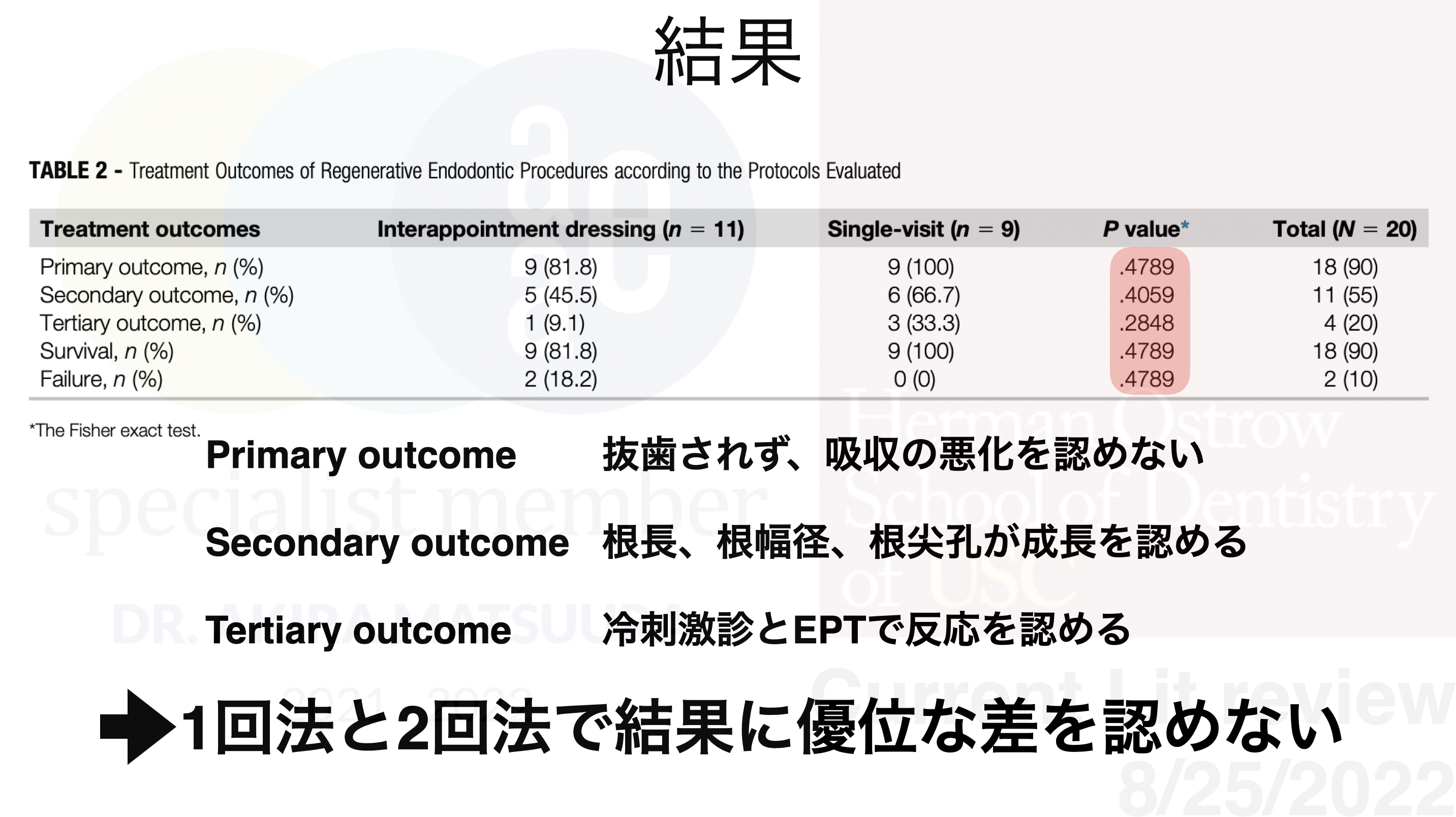
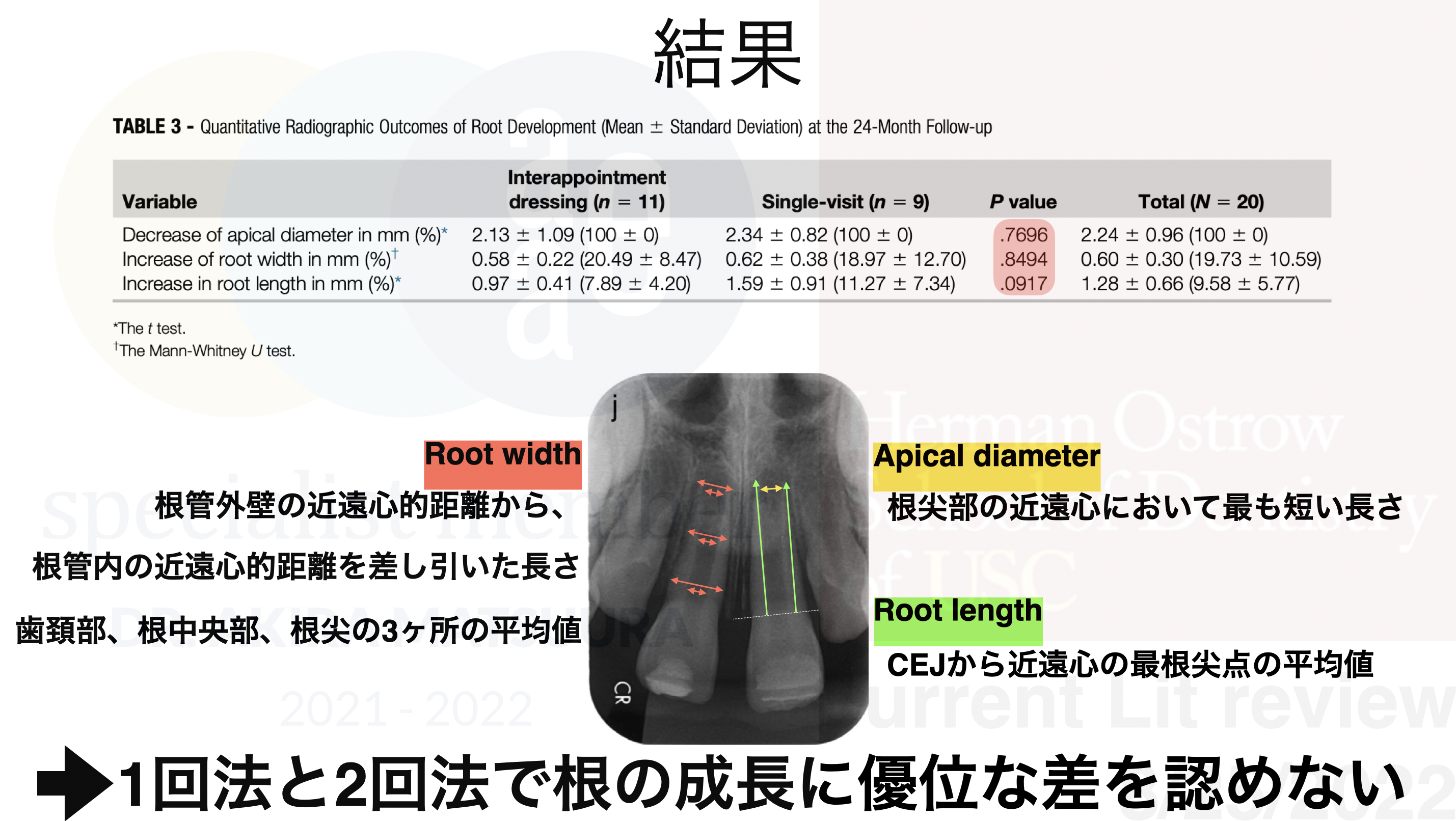

ということで1回法でも2回法でも結果に差がない。
が、
この1本しか文献がなく、
歯頚部バリアについての考察が少ない(歯頚部バリア =水酸化カルシウム製剤、2%クロルヘキシジンジェル、酸化亜鉛を混和したものを使用し、MTAやBCパテ、Biodentineを利用しない理由が不明)、
n数が少なく、差がなかったというより、優位な差がない程度のサンプル数しか揃っていない?可能性、
薬液などを変えて、ランダム化などを行って結果を検討すべき、
であるものの、
もはや麻酔薬については議論する必要がなさそう(敢えてスキャンドネストを使う理由がない)、
ということで、
1回法と2回法で治療の結果に差が出ていなかった。これは、かつてのApexificationと同じ結果だ。
昔、MTAでApexificationを1回でやる!という考えはなかったが、現在はそちらの方が支配的だろう。
そして、RegenerationをキシロカインでもOKなら、この治療がどれだけ楽か…
これだけでもRevolutionと言えるかもしれない。
さて、以上の事実を患者さんに説明した。
すると、
学会のガイドラインに裏付けされていない治療内容には不安が残るので、2回法でお願いします
という回答であった。
ということで、うちの歯科医院では珍しく2回法の治療となった。
⭐︎この後、臨床動画が出てきます。不快感を感じる方は視聴をSkipしてください。
#9 Regeneration 1回目(2023.11.29)
AAE Clinical Considerations for a Regenerative Procedure Revised 5/18/2021
によれば、1回目の治療内容は以下だ。
First Appointment
① Local anesthesia, dental dam isolation and access.
② Copious, gentle irrigation with 20ml NaOCl using an irrigation system that minimizes the possibility of extrusion of irrigants into the periapical space (e.g., needle with closed end and side-vents, or EndoVac™). Lower concentrations of NaOCl are advised [1.5%-3% NaOCl (20mL/canal, 5 min) and then irrigated with saline or EDTA (20 mL/canal, 5min), with irrigating needle positioned about 1 mm from root end, to minimize cytotoxicity to stem cells in the apical tissues.
③ Dry canals with paper points.
– Place calcium hydroxide or low concentration of triple antibiotic paste. If the triple antibiotic paste is used: 1) consider sealing pulp chamber with a dentin bonding agent [to minimize risk of staining] and 2) mix 1:1:1 ciprofloxacin: metronidazole: minocycline to a final concentration of 1-5 mg/ml. Triple antibiotic paste has been associated with tooth discoloration. Double antibiotic paste without minocycline paste or substitution of minocycline for other antibiotic (e.g., clindamycin; amoxicillin; cefaclor) is another possible alternative as root canal disinfectant. Clinicians should be aware that studies have been done using higher concentrations of TAP/DAP, but a recommendation to a higher concentration can’t be made at this time due to limited studies.
– Deliver into canal system via syringe
– If triple antibiotic is used, ensure that it remains below CEJ (minimize crown staining).
– Seal with 3-4mm of a temporary restorative material such as Cavit™, IRM™, glass-
ionomer or another temporary material. Dismiss patient for 1-4 weeks.
1回目の治療をまとめると、
ヒポクロ20mlとEDTA 20mlで洗浄しろ
ということだ。
そして、洗浄後に水酸化カルシウムで貼薬する。
水酸化カルシウムは触れた部分しか殺菌できないが、なぜかこの手の治療の場合は、根管全体に浸さずに根管の半分程度でいいという意見が多い。
全く理解ができない部分だ。
Bose, Hargreaves 2009 A Retrospective Evaluation of Radiographic Outcomes in Immature Teeth With Necrotic Root Canal Systems Treated With Regenerative Endodontic Procedures
When Ca(OH)2 was radiographically restricted to the coronal half of the root canal system, it produced better results than when it was placed beyond the coronal half.
When Ca(OH)2 was radiographically restricted to the coronal half of the root canal system, the median percentage increase in dentinal wall thickness was 53.8%, as compared with a 3.3% increase when it was placed beyond coronal half (ie, into the apical half of the root canal system).
ということで根管口の半分以上は貼薬しないほうがいいということがわかる。
これを考慮して、ヒポクロ、EDTAで洗浄して貼薬し、上述のように水酸化カルシウムを置いて綿球を入れてCavitonで仮封した。
術後にPAを撮影した。

この後、1ヶ月時間をおいて2回目の治療となった。
#9 Regeneration 2回法(2024.1.5)
AAE Clinical Considerations for a Regenerative Procedure Revised 5/18/2021
によれば2回目の治療内容は以下だ。
Second Appointment (1-4 weeks after 1st visit)
Assess response to initial treatment. If there are signs/symptoms of persistent infection, consider additional treatment time with antimicrobial, or alternative antimicrobial.
① Anesthesia with 3% mepivacaine without vasoconstrictor, dental dam isolation.
② Copious, gentle irrigation with 20ml of 17% EDTA.
③ Dry with paper points.
④ Create bleeding into canal system by over-instrumenting (endo file, endo explorer) (induce by rotating a pre-curved K-file at 2 mm past the apical foramen with the goal of having the entire canal filled with blood to the level of the cemento–enamel junction). An alternative to creating of a blood clot is the use of platelet-rich plasma (PRP), platelet rich fibrin (PRF) or autologous fibrin matrix (AFM).
⑤ Stop bleeding at a level that allows for 3-4 mm of restorative material.
– Place a resorbable matrix such as CollaPlug™, Collacote™, CollaTape™ over the
blood clot if necessary and white MTA as capping material.
– A 3–4 mm layer of glass ionomer (e.g. Fuji IX™, GC America, Alsip, IL) is flowed gently over the capping material and light-cured for 40 s. MTA has been associated with discoloration. Alternatives to MTA (such as bioceramics or tricalcium silicate cements [e.g., Biodentine®, Septodont, Lancasted, PA, USA, EndoSequence® BC RRM-Fast Set Putty, Brasseler, USA]) should be considered in teeth where there is an esthetic concern.
– Anterior and Premolar teeth – Consider use of Collatape/Collaplug and restoring with 3mm of a nonstaining restorative material followed by bonding a filled composite to the beveled enamel margin.
– Molar teeth or teeth with PFM crown – Consider use of Collatape/Collaplug and restoring with 3mm of MTA, followed by RMGI, composite or alloy.
麻酔に対しては言及した通りだ。
スキャンドネストではマネージメント不可能だ。
なので、私はキシロカインを使用した。
また、③のPaper Pointで根管を乾燥するという行為も難しい。
乾燥しないな…などど言っているとエピネフリンが効いて止血してくれる。
するとこの治療の目的である、
血液と共に幹細胞を根管に導入することができなくなる。
目的を考えて行動しなければならない。
ということで、EDTAで水酸化カルシウムを洗浄するように根管内を洗って、ペーパーポイントで便宜的に乾燥し、ファイルで根尖部を突き、出血を促した。
CEJ付近の位置まで出血を誘導てきたので問題ないだろう。
その後、血液の上に、Colaplugを置き、Biodentine, CRで充填した。

術後にPAを撮影した。

このPAを読み解くと以下だ。

CBCTも撮影した。
問題はないだろう。
さて私が考える、Regenerationだが、あくまでもこれはApexificationの一部だと私は考える。
真の再生など起きない。
その意味では、これも、再生 “的” 療法と言えるかもしれない。
次回は半年後である。
また状況をお伝えしたい。